
Chapter 55: Ischemia
Arterial Dissection
Dissection of the cervicocranial carotid and vertebral arteries is an uncommon but increasingly recognized cause of cerebral infarction. Dissection accounts for approximately 5% of ischemic strokes in young adults, occurring most commonly in persons between 30 and 50 years of age.73 The infarctions associated with dissection are thought to be mostly thromboembolic in origin73; thus early recognition of dissection is important so that prophylactic anticoagulation can be instituted. The clinical presentation of extracranial internal carotid artery (ICA) dissection varies. Often a symptom complex of unilateral headache and an incomplete Horner's syndrome secondary to impairment of the periarterial sympathetic plexus, with or without monocular blindness, can be detected.65 Vertebral artery dissection can cause visual, vestibular, and gait disturbances, as well as syncope. Symptoms may develop precipitously, but often progressive neurological deficits evolve over 2 to 3 days, which reflects the territory of the affected vessel. Massive infarction occurs in only 10% to 20% of patients. Most recover completely, and recurrence is infrequent.58
Although multiple causes, including atherosclerosis, arteritis secondary to migraine, and congenital anomalies such as a vascular loop, have been proposed, most dissections occur spontaneously in morphologically normal vessels. Mild trauma, such as chiropractic manipulation, coughing, sneezing, and head turning, is implicated in a minority of cases, more commonly with vertebral artery disease.119 Interestingly, 23% to 30% of these patients have fibromuscular dysplasia at examination.82
Dissection of the ICA is common (80%), with a predilection for the right side. The tear usually occurs 2 cm or more beyond the origin of the ICA and terminates before or at the entry into the petrous bone, where the rigid bony canal tends to limit further dissection.30 Vertebral artery dissection occurs less frequently (20%), usually arising at the craniocervical junction. Approximately one third of patients show involvement of multiple arteries53,65,82 (Figure 55-24); these patients are more likely to have fibromuscular dysplasia. By intraarterial angiography, 80% of vessels show stenosis and 20% demonstrate occlusion in cases of dissection of the cervical great vessels.65 Again, recovery is the rule, and in one representative series, 63% of the cases normalized and 26% improved on follow-up angiography over several months.82
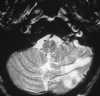  |
| Figure 55-24 A 21-year-old woman with syncopal episodes seen in the emergency room. A, T2-weighted axial MRI shows abnormal signal involving the PICA territory. Also note the collar of high signal intensity involving the left ICA at its entrance to the petrous canal. B, Left common carotid artery intraarterial injection shows severe segmental narrowing of the left ICA consistent with dissection (arrow). Left vertebral artery dissection was also found (not illustrated). |
Intracranial carotid artery dissection, although rare, often occurs in a setting of severe head trauma in young patients and is characterized clinically by the evolution (over several days) of severe headache and massive stroke. Occasionally, intracranial dissection can be associated with fibromuscular dysplasia, moyamoya disease, and cystic medial necrosis, but most vessels examined are histologically normal.58
Standard spin-echo MRI in combination with MRA has been shown to be a reliable, noninvasive method for evaluating cervical artery dissection.30,80 On standard spin-echo sequences, intramural hematomas are best seen on axial images as regions of altered, crescentic signal within the vessel wall; the signal intensity changes with the age of the clot. Care must be taken not to mistake fat within the carotid sheath for hematoma (fat saturation sequences can help in this regard). Signs of cerebral artery infarction in the distribution of the involved artery must be sought. In a recent study, 3D TOF MRA was shown to have a sensitivity and specificity of 95% and 99%, respectively, for carotid artery dissection.80 An apparent increase in the external artery diameter, observed in 95% of the patients, was the best indicator of dissection. The pseudoenlargement is a result of intramural hematoma (methemoglobin) surrounding the dissection (Figure 55-25).30,80 In addition, flow within a dissected vessel is typically of higher signal intensity than the surrounding hematoma, thus allowing visualization of arterial patency.80 Although the ICA narrowing is often seen at MRA, this sign is less specific (93%) because it is also observed in a variety of other conditions, such as atherosclerotic stenosis, vessel hypoplasia, and dysplasia. MRA is less useful in the evaluation of vertebral artery dissection because of its poor specificity of 20%.80 This is thought to be due to the considerable normal variation in the caliber of the vertebral artery, thus rendering it difficult to assess for intramural hematoma or the less specific sign of stenosis.80 Therefore MRA used in combination with the source images and standard spin-echo sequences is useful for both the diagnosis and follow-up of extracerebral dissection.
  |
| Figure 55-25 A 60-year-old man with a history of cluster headaches and Cafergot abuse presents with amaurosis fugax. A, Proton density–weighted axial image obtained at the skull base shows an eccentric high signal intensity ring of methemoglobin involving the right ICA (black arrow). Note the normal signal void of the left ICA (white arrow). B, 3D TOF MRA shows pseudoenlargement of the right ICA external diameter (white arrows) as a result of subacute intramural hematoma. |
~ Previous ~ Next ~
~ Back to Chapter Index ~
~ Back to Magnetic Resonance Imaging main page ~